All types of Major (Right hepatectomy, Left Hepatectomy, Central hepatectomy) and minor liver resections (left lateral segmentectomy, Right posterior sectionectomy etc) are performed for different benign (Adenoma, FNH, Hemangioma etc.) and malignant Tumors of the liver (Hepatocellular carcinoma, Colorectal metastasis, Nets etc.). Laparoscopic Marsupialisation is commonly performed for hydatid cyst and large cysts of Polycystic liver disease, Spleenectomy + Proximal Spleenorenal shunt (PSRS) is routinely performed for portal Hypertension (NCPF/ EHPVO).
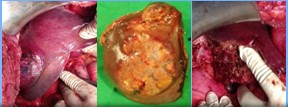
Right Hepatectomy performed for a 75-year-old male with a large right lobe (10 x12cm) liver tumor (Hepatocellular carcinoma)
Left lateral Segmentectomy (seg II & III) performed for a 47-year-old cirrhotic patient with left lobe liver tumor (7×8 cm, Hepatocellular carcinoma)
Indocyanine Green being used during Right posterior Sectionectomy in a patient with severe Right liver injury”. “ICG was used for the first time in orissa during different major and minor Liver resections at LIGG hospital.
Pancreatic Surgery
The HPB unit at LIGG hospital has carried out > 500 major pancreatic resections with results comparable with the best centers in the world. Surgical treatment is offered to patients with all types of Benign (IPMN, CNOP, Insulinoma, Neuoroendocrine tumors etc) and malignant tumors (Adenocarcinoma of Head of pancreas and Periampullary cancers) of pancreas with radical surgery like Whipple’s pancreatico-duodenectomy / Distal pancreatectomy + Spleenectomy etc.
Whipple’s pancreatico-duodenectomy in a 18yr old child with large benign pancreatic head Tumor
Roux En Y LPJ in a patient with Chronic calcific pancreatitis
We believe in a team and guided approach to different complications of acute pancreatitis like Necrotising pancreatitis, Pancreatic ascites, pleural effusion pseudocyst of pancreas , psedoaneurysm and pancreatic fistula with Percutaneous Drainage (USG/CT guided) , Laparoscopic / Open Necrosectomy, Irrigation & Drainage, Laparoscopic and open cystogastrostomy etc. All patients with chronic pancreatitis and pain abdomen are managed surgically with Roux En Y lateral pancreatico-jejunostomy with head coring and resectional procedure like DPS / whipple’s procedure for Tail and Head predominant disease respectively.
KEEP YOUR PANCREAS HEALTHY
Acute pancreatitis – is a life threatening conditions in which pancreas become inflamed and release toxic substance that affects different systems of the body, usually related to alcohol intake or Gall stone induced pancreatitis. Milder cases are usually managed conservatively with medicines, but patients with severe necrotising pancreatitis with failure to best medical and ICU care undergo surgery to remove the necrosed part of pancreas and drainage of the peripancreatic infected fluid collection.
Chronic pancreatitis – is a reversible fibrosis of pancreatic parenchyma, usually linked to chronic alcohol intake, smoking or tropical calcific pancreatitis. This leads to pancreatic atrophy, dilated pancreatic duct and multiple pancreatic ductal calculi. Patients present with severe upper abdominal pain radiating to back, typically after taking spicy food or binge drinking. All patients with recurrent pain are managed with pancreatic drainage procedure like LPJ (lateral pancreatico-jejunostomy) or pancreatic resection.
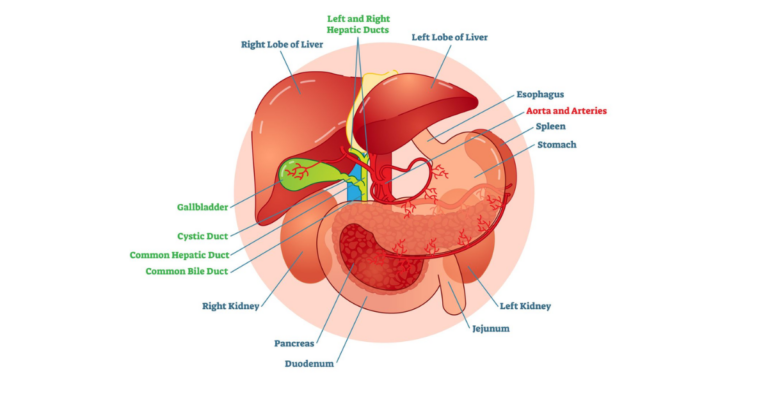
Biliary Tract Surgery
Biliary tract Stone disease
Gall bladder Stones and its complications like Empyema, Mucocele, acute cholecystitis, Mirrizi’s syndrome etc – Managed by Laparoscopic cholecystectonmy
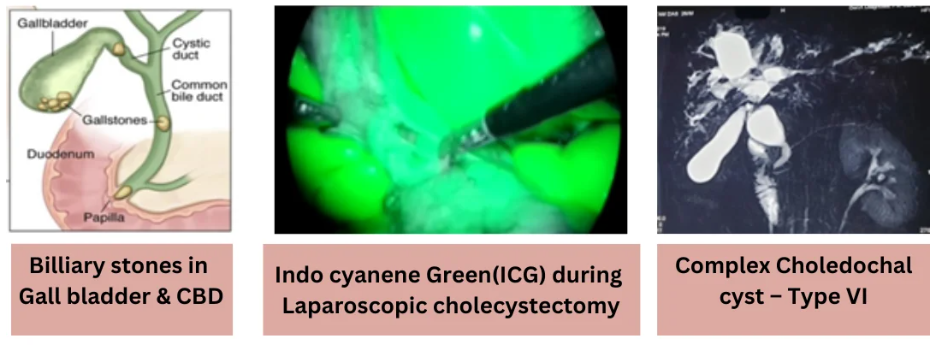
Common bile duct (CBD) and intrahepatic stones – treated with Laparoscopic CBD exploration with intra-operative Flexible choledochoscopy (with mechanical and Laser Lithotripsy – one of it’s kind in orissa since 2009), Complicated and recurrent cases managed with billiary bypass surgery ( choledocho-duodenostomy & Roux en Y Hepatico-jejunostomy).
Complicated benign biliary disorders
Choledochal cysts (both intra & Extrahepatic) – Excision + Roux En Y Hepaticojejunostomy.
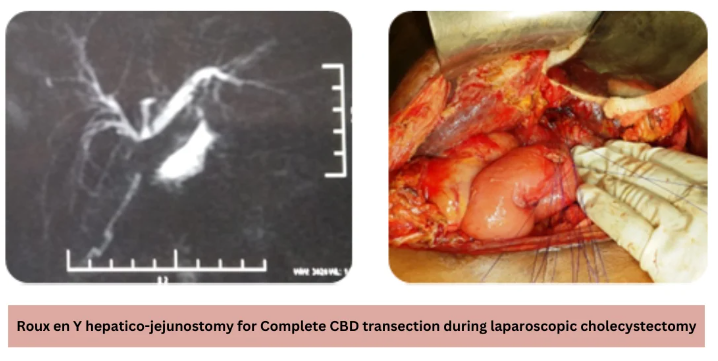
Bile duct Injury and benign billiary strictures – managed in coordination with the Medical Gastroenterology Department depending on severity and nature of lesion like Endoscopic Billiary stenting for mild injury to Roux en Y hepatico-jejunostomy for complex injuries.
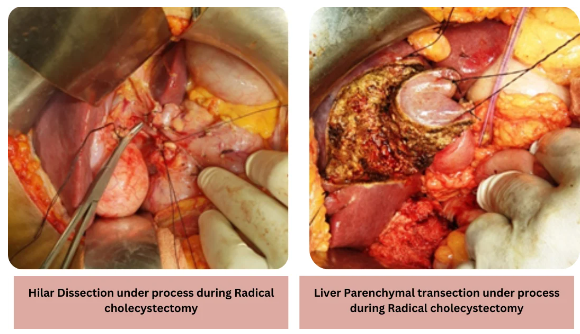
Biliary tract (Bile duct and gall bladder) cancer
Gall Bladder Cancer – Radical cholecystectomy with wedge resection / Segment IVB &V resection of Liver is routinely performed.
Mid and distal CBD cancer – Whipple’s pancreaticoduodenectomy is performed.
Hilar and intrahepatic Bile duct cancer – usually treated with Hilar Excision with Right / Left hepatectomy ( along with vascular resection of Portal vein / hepatic artery for advanced lesions).
Patients who have inoperable diseases are offered various palliative measures like stenting or segment III billiary bypass procedures.